The Silent Threat: Why Cystic Lung Lesions Demand a New Diagnostic Approach
For decades, medical professionals have relied on standard imaging to identify lung cancer. However, a group of “hidden” tumors—neoplasms arising within pulmonary cystic airspaces—is challenging the status quo. These lesions are notoriously difficult to spot, often masquerading as benign conditions like emphysematous bullae or simple inflammatory changes.
With only 1% to 4% of non-small cell lung cancers originating in these airspaces, they are rare, yet dangerous. Because they are often misdiagnosed, patients frequently present with advanced-stage disease. As we move toward more personalized pulmonary care, the medical community is shifting its focus toward high-precision diagnostic tools to catch these “cysts in disguise” before it is too late.
The Diagnostic Dilemma: Why Conventional Biopsy Fails
The primary hurdle in diagnosing cystic lung lesions is their anatomy. The malignant tissue is often minor, eccentric, or tucked away next to air-filled spaces. Standard CT-guided transthoracic biopsies—while effective for solid tumors—often return non-diagnostic results for cystic lesions because the needle may pass through the air space without capturing the critical, thickened wall of the tumor.
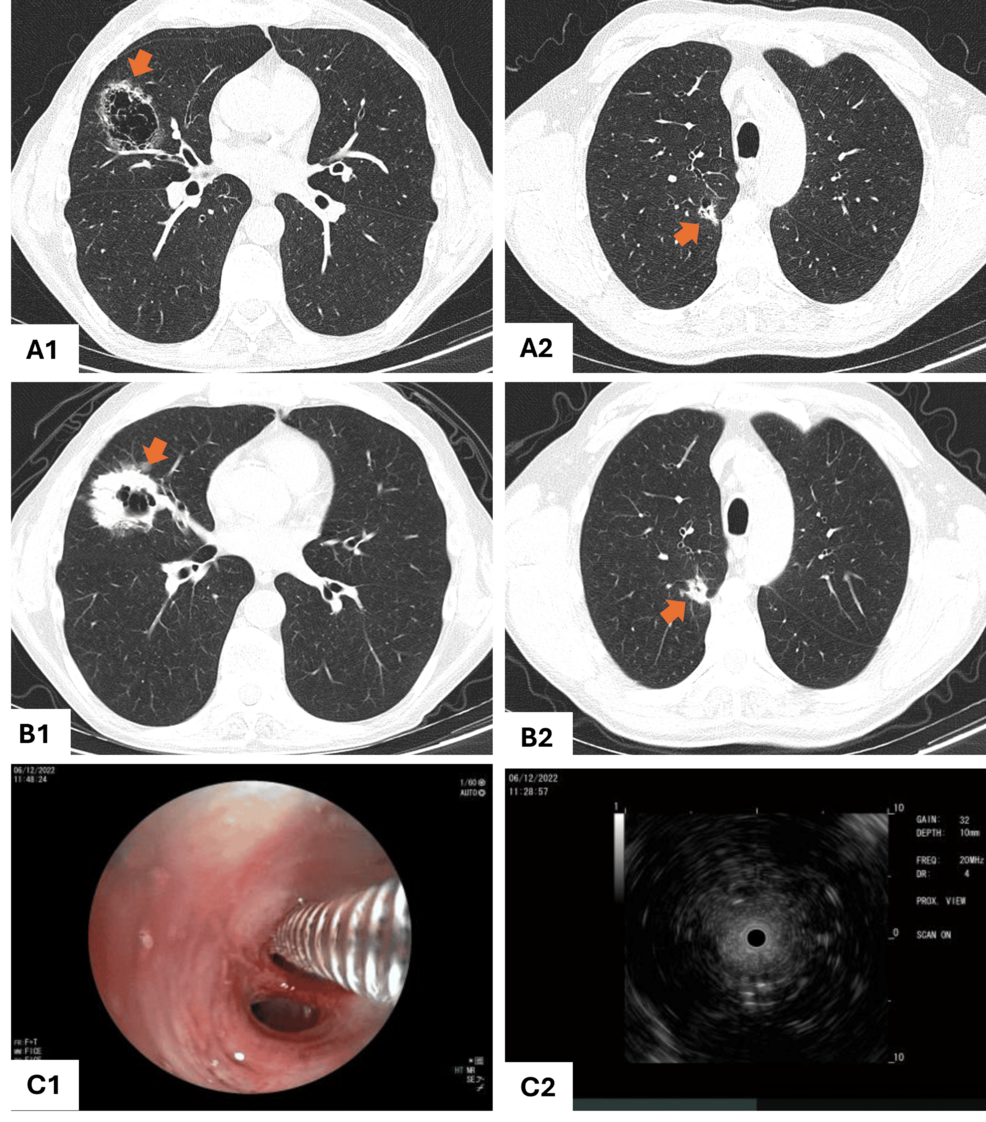
In a recent clinical case, a 61-year-old high-risk smoker underwent a CT-guided biopsy that failed to provide a definitive answer. It wasn’t until a secondary, more targeted approach was utilized that the malignancy was confirmed. This underscores a growing trend in pulmonology: the need for a multimodal diagnostic strategy.
The Rise of Radial Endobronchial Ultrasound (r-EBUS)
As diagnostic technology evolves, radial endobronchial ultrasound (r-EBUS) is emerging as a game-changer. Unlike percutaneous biopsies, which carry a higher risk of pneumothorax (collapsed lung) or hemorrhage, r-EBUS provides a minimally invasive, real-time look inside the airways.
By using a miniature ultrasound probe, physicians can navigate the bronchial tree to locate the lesion with pinpoint accuracy. The “concentric probe-within-lesion” pattern allows doctors to visualize the solid component of a cystic lesion, ensuring the biopsy sample is representative and accurate. This technology is becoming the gold standard for navigating the complex geography of peripheral lung nodules.
Future Trends: AI and Early Detection
Looking ahead, the integration of Artificial Intelligence (AI) into thoracic imaging is set to revolutionize how we track these lesions. AI algorithms are currently being trained to recognize the subtle, “spiculated” margins and progressive wall thickening that the human eye might miss in early-stage scans.
the inclusion of atypical pulmonary cysts in the Lung-RADS (Lung Imaging Reporting and Data System) framework provides a structured pathway for clinicians. This shift ensures that cystic lesions are no longer treated as “incidental findings” but as high-priority targets for active surveillance.
Frequently Asked Questions
Are all cystic lung lesions cancerous?
No. Most cystic lesions are benign results of prior infections or emphysema. However, because they can mask underlying malignancy, they require careful monitoring by a pulmonologist.
Why did my biopsy come back non-diagnostic?
Cystic lesions are difficult to sample because the cancer is often localized to a specific, small part of the cyst wall. If the needle misses that specific area, the biopsy will show only normal tissue or fluid.
Is r-EBUS painful?
The procedure is performed under sedation, meaning the patient is comfortable. It is generally considered safer and less invasive than surgery or large-needle percutaneous biopsies.
Have you or a loved one navigated the complexities of lung health screenings? Share your experience in the comments below, or subscribe to our newsletter for the latest updates on medical technology and lung health.
Related reading