
Medicaid’s Prescription Drug Challenge: Balancing Access, Cost and Innovation
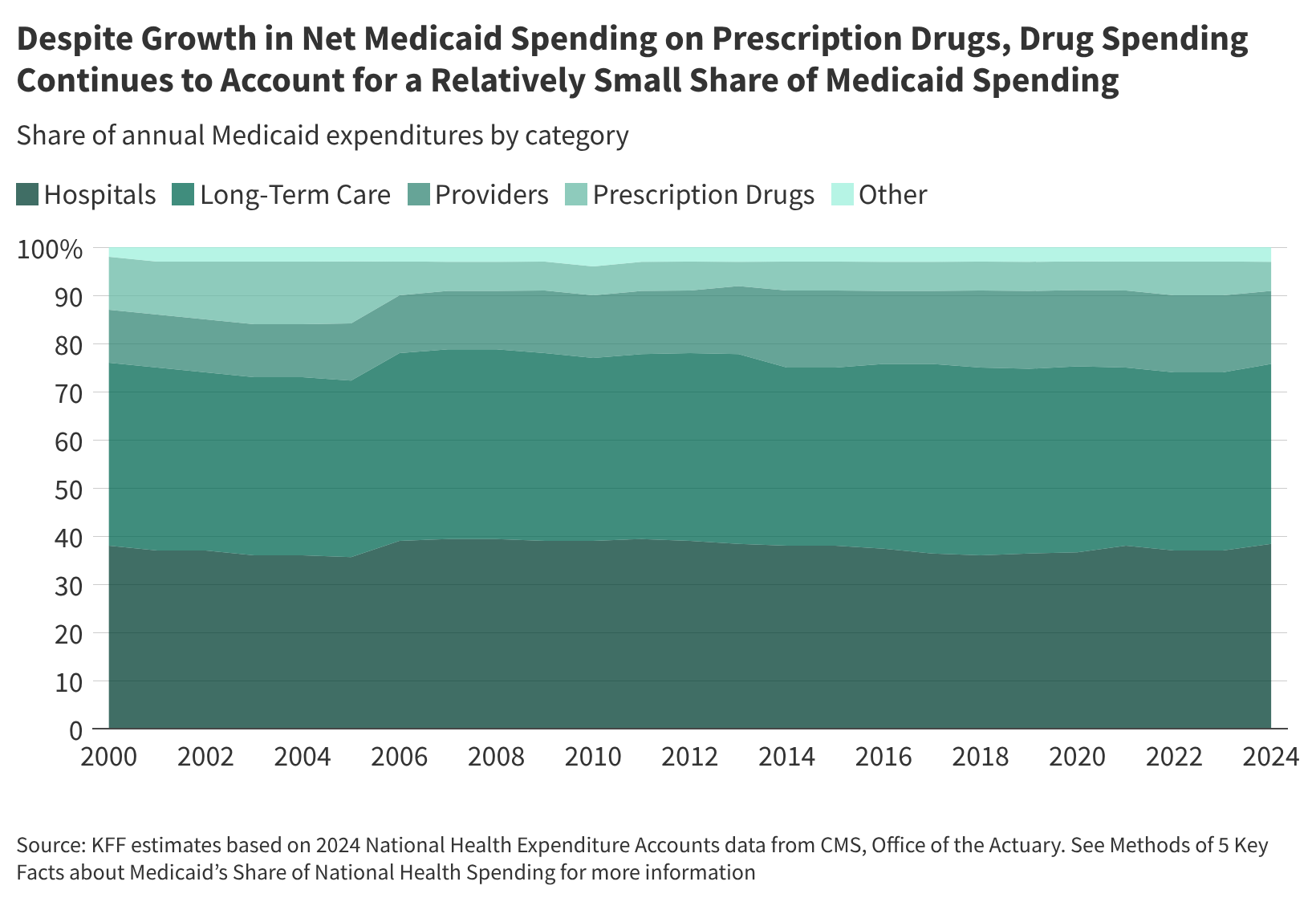
Medicaid, covering roughly one in five Americans, faces a growing challenge in managing prescription drug costs. Although representing only 6% of overall Medicaid spending in 2024 – significantly less than hospital (38%) and long-term care (37%) costs – the emergence of expensive modern drugs, including GLP-1s and cell and gene therapies, is putting increasing pressure on state and federal budgets.
The Rising Cost of Innovation
The introduction of innovative, high-cost drugs is a primary driver of increased Medicaid spending. These therapies, while potentially curative for rare diseases or offering significant benefits for chronic conditions, strain state budgets. Simultaneously, a more tenuous fiscal climate, coupled with federal funding shifts, necessitates careful management of pharmacy costs.
Affordability for Enrollees: A Core Medicaid Principle
A key tenet of Medicaid is ensuring access to affordable prescription drugs for low-income individuals. Federal law limits out-of-pocket costs for enrollees to nominal amounts – up to $4 for preferred drugs and $8 for non-preferred drugs for those with incomes at or below 150% of the federal poverty level. Despite these limits, even small costs can be prohibitive for some families. Over two-thirds of Medicaid enrollees took prescription medication in the past year, but 10% reported delaying or rationing prescriptions due to cost, a rate slightly higher than privately insured adults (8%).
State-Level Variation in Pharmacy Benefit Management
States employ diverse strategies to administer the pharmacy benefit within Medicaid. While not mandated, all states cover prescription drugs, but the approach varies. As of July 2025, eight out of 42 states contracting with managed care organizations (MCOs) deliver the pharmacy benefit through fee-for-service, while the remaining states include it in capitation rates paid to MCOs. Many states also contract with Pharmacy Benefit Managers (PBMs) to manage or administer the pharmacy benefit, though PBMs are facing increased scrutiny and reform efforts.
Did you know? As of July 1, 2023, fewer than half of states required prescription drug cost-sharing for non-exempt enrollees.
The Complexities of Medicaid Drug Payments
Medicaid drug payments are determined by a complex formula. The total cost is based on the amount paid to the pharmacy, less rebates received from manufacturers. Rebates are a crucial component, stemming from the Medicaid Drug Rebate Program (MDRP) and supplemental agreements negotiated by states. States reimburse pharmacies based on the ingredient cost of the drug and a dispensing fee, subject to federal regulations and state-specific policies. The final cost is then offset by rebates.
Utilization Management: Balancing Access and Cost Control
States utilize a range of utilization management strategies to control prescription drug expenditures. These include prior authorization, preferred drug lists (PDLs), step therapy, prescription limits, and medication therapy management (MTM) programs. These strategies aim to ensure appropriate medication use and cost-effectiveness, while maintaining access for enrollees. States are continually updating and expanding these initiatives, with many focusing on high-cost specialty drugs.
Future Trends and Potential Impacts
Several factors will likely shape Medicaid’s prescription drug landscape in the coming years:
- Increased Adoption of Value-Based Agreements (VBAs): States are increasingly exploring VBAs, where manufacturers offer rebates based on the real-world performance of their drugs.
- Federal Initiatives and Payment Models: New federal initiatives, including those focused on cell and gene therapies, could impact state Medicaid programs, though the extent of the savings and responses from states and manufacturers remain unclear.
- Continued Scrutiny of PBMs: Ongoing efforts to increase PBM transparency and oversight at both the state and federal levels could reshape the pharmacy benefit management landscape.
- Expansion of Specialty Drug Coverage: The increasing prevalence of specialty drugs, particularly for chronic conditions, will necessitate innovative strategies to manage costs and ensure access.
The ongoing tension between providing access to innovative therapies and controlling costs will continue to define Medicaid’s prescription drug policy. States will require to balance the need for affordability with the desire to offer enrollees the latest medical advancements.
Key Medicaid Drug Pricing Terms
AAC: Actual acquisition cost, the price pharmacies pay for drugs.
AMP: Average manufacturer price, used to calculate drug rebates.
FUL: Federal upper limit, a reimbursement cap for some drugs.
MDRP: Medicaid Drug Rebate Program, a key cost-containment mechanism.
Frequently Asked Questions (FAQ)
What is the Medicaid Drug Rebate Program (MDRP)?
The MDRP requires drug manufacturers to provide rebates to state Medicaid programs in exchange for coverage of their drugs.
How do states manage prescription drug costs in Medicaid?
States use a variety of strategies, including rebates, utilization management techniques (prior authorization, PDLs), and negotiating supplemental rebates with manufacturers.
What role do Pharmacy Benefit Managers (PBMs) play in Medicaid?
PBMs often manage or administer the pharmacy benefit for Medicaid programs, negotiating rebates and processing claims.
Pro Tip: Stay informed about state-specific Medicaid policies regarding prescription drug coverage and utilization management to understand your options and potential costs.
To learn more about Medicaid and prescription drug coverage, explore additional resources on the Kaiser Family Foundation website and the Medicaid.gov portal.
What are your thoughts on the future of Medicaid drug pricing? Share your comments below!