The Brain’s Unexpected Resilience: How Stroke Recovery is Being Rewritten with AI
A groundbreaking study published in The Lancet Digital Health is reshaping our understanding of stroke recovery. Researchers at the USC Mark and Mary Stevens Neuroimaging and Informatics Institute (Stevens INI) have discovered that the brain doesn’t just adapt around damage after a stroke – it appears to actively “rejuvenate” healthy areas to compensate, a process revealed through the power of artificial intelligence.
Unlocking Neuroplasticity with Deep Learning
For years, neuroplasticity – the brain’s ability to reorganize itself by forming new neural connections throughout life – has been a central focus of stroke rehabilitation. But, pinpointing the specific mechanisms and extent of this reorganization has remained a challenge. This new research, part of the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA) Stroke Recovery Working Group, changes that.
The study analyzed brain scans from over 500 stroke survivors across eight countries, utilizing deep learning models trained on tens of thousands of MRI scans. This allowed researchers to estimate the “brain age” of different regions, identifying a surprising pattern: larger strokes accelerate aging in the damaged hemisphere, while the opposite, undamaged side appears structurally “younger.”
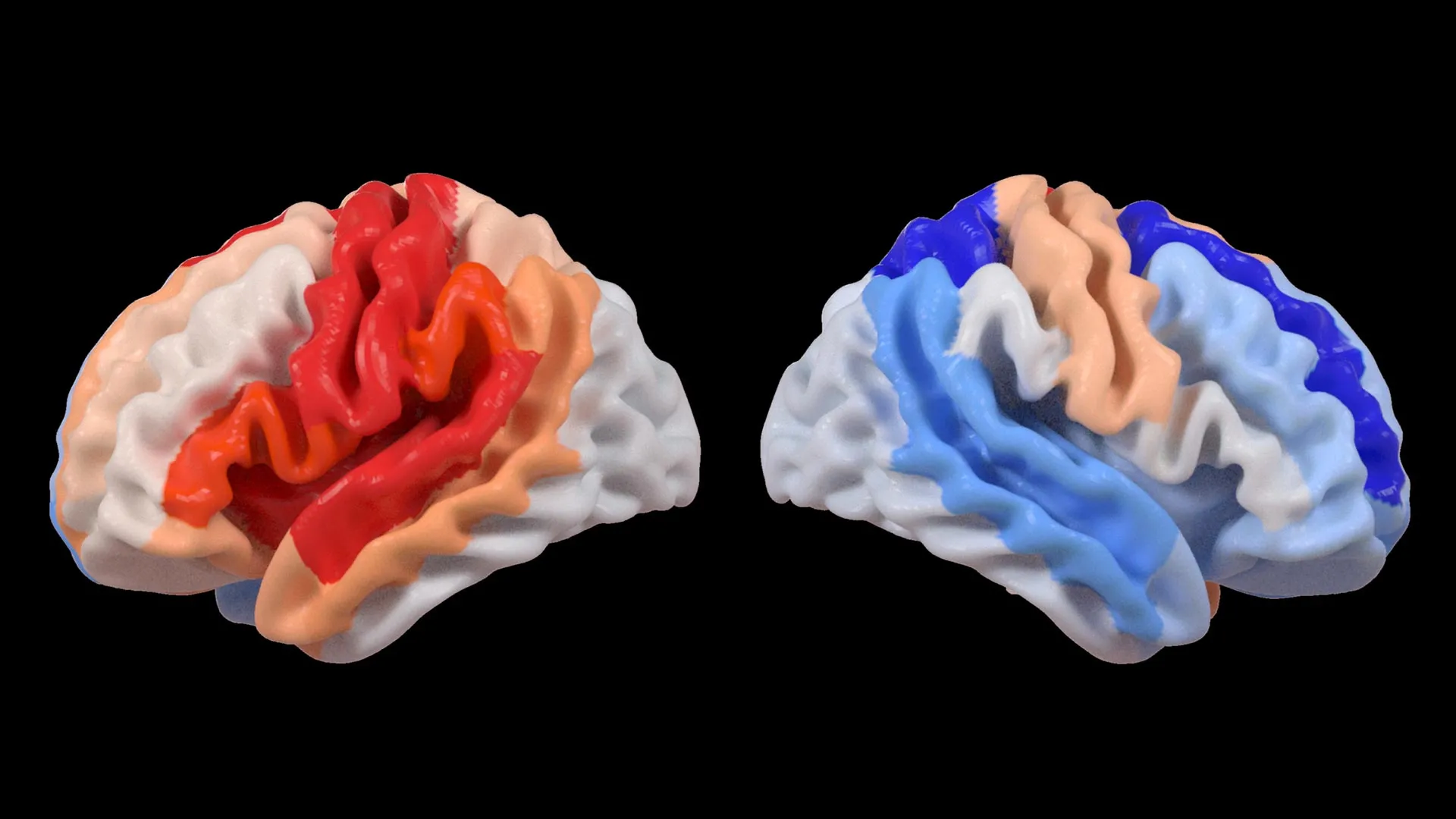
The Contralesional Shift: A Brain’s Counterintuitive Response
“We found that larger strokes accelerate aging in the damaged hemisphere but paradoxically make the opposite side of the brain appear younger,” explains Hosung Kim, PhD, associate professor of research neurology at the Keck School of Medicine of USC. This “youthfulness” isn’t simply a passive observation; it’s strongly correlated with the frontoparietal network, a crucial area for motor planning, attention, and coordination.
This phenomenon, dubbed the “contralesional shift,” suggests the brain is actively reorganizing itself, essentially bolstering healthy networks to take on the functions lost due to injury. Researchers used a measure called the brain-predicted age difference (brain-PAD) to quantify this effect, finding that more severe movement impairments were linked to more pronounced “youthful” patterns in the undamaged hemisphere.
From Global Collaboration to Personalized Rehabilitation
The scale of this study is unprecedented, thanks to ENIGMA’s collaborative network spanning 34 research sites. By pooling data from hundreds of stroke survivors worldwide, researchers were able to detect subtle patterns of brain reorganization that would have been impossible to identify in smaller studies. This highlights the power of large-scale data and international collaboration in advancing neuroscience.
Arthur W. Toga, PhD, director of the Stevens INI, emphasizes the potential for personalized rehabilitation strategies. “By pooling data…and applying cutting-edge AI, we can detect subtle patterns…These findings of regionally differential brain aging…could eventually guide personalized rehabilitation strategies.”
Future Trends: Tracking Brain Age for Optimized Recovery
The research team is now focused on longitudinal studies, tracking patients over time to understand how brain aging patterns evolve throughout the recovery process. This could lead to the development of biomarkers – measurable indicators of biological states – that predict an individual’s potential for recovery and inform tailored treatment plans.
Imagine a future where MRI scans aren’t just used to diagnose stroke damage, but to predict how a patient’s brain will reorganize itself and respond to different therapies. This level of personalization could dramatically improve outcomes and quality of life for stroke survivors.
Did you realize? The brain’s ability to reorganize isn’t limited to stroke recovery. Neuroplasticity plays a role in learning new skills, recovering from traumatic brain injuries, and even adapting to sensory loss.
FAQ
Q: Does a “younger” brain age always mean better recovery?
A: Not necessarily. The study suggests it reflects the brain’s attempt to compensate, but doesn’t guarantee full functional recovery.
Q: What is the ENIGMA Stroke Recovery Working Group?
A: It’s an international research collaboration focused on understanding the genetic and environmental factors influencing stroke recovery.
Q: How was “brain age” measured in this study?
A: Researchers used deep learning models to analyze MRI scans and predict the age of different brain regions, comparing it to the participant’s actual age.
Q: What role does AI play in this research?
A: AI, specifically deep learning, allowed researchers to analyze vast amounts of MRI data and identify subtle patterns of brain reorganization that would be impossible to detect manually.
Pro Tip: Engaging in consistent rehabilitation exercises, even months after a stroke, can support maximize neuroplasticity and improve functional outcomes.
Want to learn more about the brain’s remarkable ability to heal? Watch this video from the Stevens INI to explore the fascinating world of neuroplasticity.
Share your thoughts on this groundbreaking research in the comments below! And be sure to explore our other articles on brain health and neurological conditions for more insights.