
The Rising Risks for Paralyzed Patients Undergoing Major Cancer Surgery
A recent study has illuminated a critical, often overlooked area of patient care: the significantly higher risk of complications faced by individuals with paraplegia undergoing major cancer surgeries. Researchers analyzing data from the National Inpatient Sample (2000-2019) found that while paraplegic patients represent a small percentage (0.2-0.3%) of those undergoing procedures like colectomy, radical hysterectomy, lung resection, gastrectomy, and pancreatectomy, they experience substantially worse in-hospital outcomes.
Understanding the Increased Vulnerability
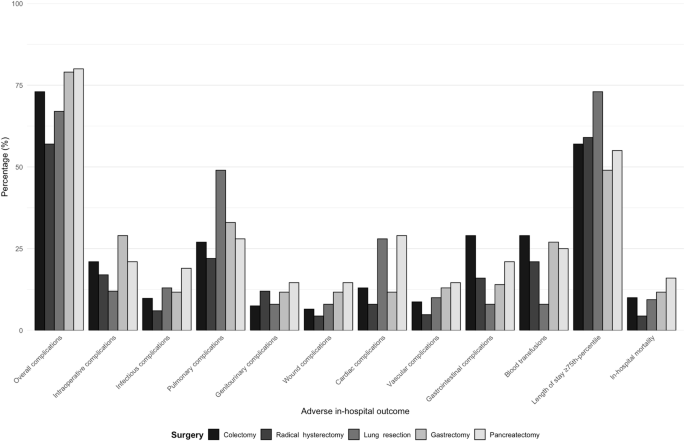
The study pinpointed a consistent pattern: paraplegia independently predicted adverse outcomes across all five surgical procedures examined. These outcomes ranged from overall complications and intraoperative issues to vascular problems and extended hospital stays. Specifically, patients with paraplegia faced a 2.4 to 4.8-fold increase in complications, and a 1.5 to 2.3-fold longer hospital stay. Perhaps most concerning, in-hospital mortality rates were 3.8 to 6.3 times higher for paraplegic patients following colectomy, lung resection, and pancreatectomy.
This increased risk isn’t simply due to the paralysis itself. The research highlighted a higher prevalence of co-occurring conditions (CCI) among paraplegic patients, particularly after lung resection and colectomy. These conditions, combined with the inherent physiological challenges associated with paraplegia – including autonomic, cardiovascular, and immune dysregulation – create a perfect storm of vulnerability.
The Impact of Neurogenic Bowel and Bladder Dysfunction
A key factor contributing to these adverse outcomes is neurogenic bowel and bladder dysfunction, common consequences of spinal cord injury. These conditions can lead to urinary tract infections, ileus, and pressure ulcers – all of which can significantly complicate post-operative recovery. Effective management of these issues requires specialized care, often lacking in general hospitals performing major cancer surgeries.
Did you know? The “Imola-Montecatone” subtotal colectomy, a procedure designed to improve bowel management in spinal cord injury patients, demonstrates a proactive approach to mitigating some of these risks. This involves using a bioabsorbable prosthesis to prevent parastomal hernias, potentially reducing complications.
Future Trends in Care: Towards Specialized Surgical Pathways
The study’s findings strongly suggest a need for a paradigm shift in how surgical care is delivered to patients with paraplegia. Several trends are likely to emerge in the coming years:
- Multidisciplinary Co-Management: Increased collaboration between surgeons, rehabilitation specialists, and spinal cord injury centers will grow standard practice. This ensures a holistic approach to pre-operative assessment, intra-operative management, and post-operative rehabilitation.
- Early Referral to Specialized Centers: For complex cases, early referral to specialized spinal cord injury centers – equipped with structured nursing protocols and rehabilitation support – will be crucial.
- Targeted Staff Education: Hospitals without dedicated SCI units will need to invest in targeted education for surgical and nursing staff, focusing on bowel, bladder, and skin care protocols specific to paraplegic patients.
- Enhanced Prehabilitation Programs: Optimizing a patient’s physical and psychological condition *before* surgery – through targeted exercise, nutritional support, and psychological counseling – can improve resilience and reduce the risk of complications.
- Data-Driven Risk Stratification: Developing more sophisticated risk stratification models that incorporate factors beyond paraplegia (such as CCI, age, and surgical complexity) will allow for more personalized care plans.
The Role of Technology and Innovation
Technological advancements are also poised to play a role. Improved monitoring systems for autonomic dysfunction, advanced wound care technologies, and telehealth solutions for remote monitoring of bowel and bladder function could all contribute to better outcomes. Research into novel surgical techniques and anesthesia protocols tailored to the unique physiological challenges of paraplegic patients is essential.
FAQ
Q: Are all cancer surgeries equally risky for paraplegic patients?
A: No. The study found the highest risk associated with colectomy, radical hysterectomy, and lung resection, with moderate risk after pancreatectomy and the least evident risk after gastrectomy.
Q: What is neurogenic bowel dysfunction?
A: It’s the impairment of bowel function due to a neurological injury, like spinal cord injury, impacting a person’s quality of life and requiring comprehensive management strategies.
Q: What can be done to reduce the risk of complications?
A: Multidisciplinary care, early referral to specialized centers, targeted staff education, and enhanced prehabilitation programs are all key strategies.
Q: Is in-hospital mortality significantly higher for paraplegic patients?
A: Yes, the study showed a 3.8 to 6.3-fold higher rate of in-hospital mortality for paraplegic patients undergoing colectomy, lung resection, and pancreatectomy.
Pro Tip: Open communication between the patient, their family, and the healthcare team is paramount. Patients should actively participate in decision-making and voice any concerns they may have.
This research underscores the urgent need for a more nuanced and proactive approach to surgical care for patients with paraplegia. By recognizing their unique vulnerabilities and implementing specialized care pathways, we can significantly improve their outcomes and quality of life.
Want to learn more about managing neurogenic bowel after spinal cord injury? Read our comprehensive guide here.