When Cancer Mimics the Unusual: Understanding Rare Metastatic Patterns
In the complex world of oncology, some metastatic patterns challenge our standard understanding of how cancer spreads. While ampullary carcinoma—a malignancy arising from the ampulla of Vater—typically follows predictable paths toward the liver, lungs, or lymph nodes, medical professionals occasionally encounter “outlier” cases that defy expectation.
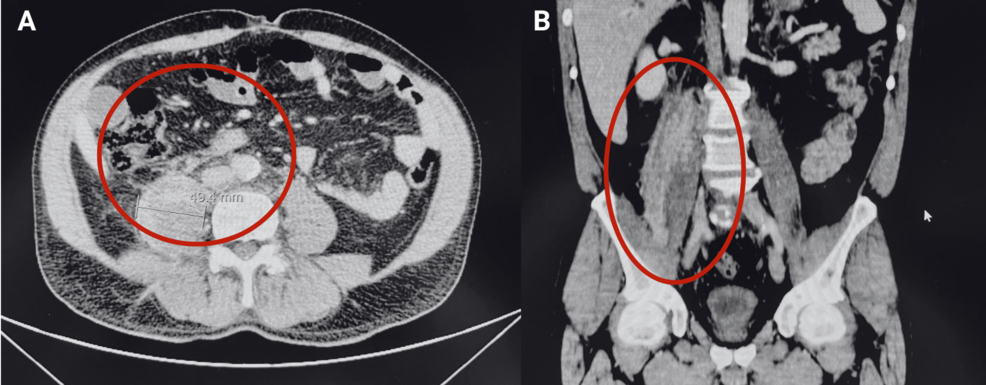
A recent clinical case involving a 67-year-old patient sheds light on an exceptionally rare presentation: metastasis to the psoas muscle. This rare occurrence serves as a vital reminder that in the presence of malignancy, atypical muscular lesions must be investigated with high clinical suspicion.
The Challenge of Ampullary Carcinoma
Ampullary carcinoma is a rare epithelial malignancy, accounting for less than 1% of all gastrointestinal cancers. With an incidence of approximately 0.59 per 100,000 persons per year, it is most frequently diagnosed in older adults and men.
Because of its specific anatomic location, the disease often presents earlier than other periampullary neoplasms, typically manifesting as painless jaundice or cholestatic liver abnormalities. While early detection can sometimes allow for curative surgery, such as a pancreaticoduodenectomy, the disease remains aggressive. Histologically, these tumors are divided into intestinal and pancreatobiliary subtypes, with the latter often carrying a more challenging prognosis.
Although skeletal muscle makes up a significant portion of body mass and is highly vascularized, it is an extremely rare site for metastasis. Scientists hypothesize that factors like local immune surveillance, metabolic conditions such as lactic acid accumulation, and high intramuscular pressure may create an “unfriendly” environment for tumor cells.
When the Psoas Muscle is Involved
The psoas muscle is a particularly unusual site for metastatic spread. When lesions appear in this area, they can easily mimic other conditions, such as hematomas, inflammatory myositis, or abscesses. This diagnostic ambiguity is why histological confirmation—usually via percutaneous biopsy—is non-negotiable for accurate staging.
In the case of the 67-year-old patient, initial imaging revealed the classic “double-duct sign”—dilation of both the common bile and pancreatic ducts—yet no clear obstructing mass was visible. It was only through advanced MRI and subsequent biopsy that the heterogeneous thickening of the right psoas muscle was confirmed as metastatic adenocarcinoma. This finding immediately shifted the treatment plan from potential surgery to palliative systemic chemotherapy, as the primary tumor was deemed locally unresectable due to its involvement with major arterial structures like the superior mesenteric artery.
Future Trends in Diagnostic Oncology
As we look to the future, the integration of high-resolution imaging and molecular profiling will likely become even more critical in identifying these “silent” metastases. The medical community is increasingly moving toward multidisciplinary evaluations where radiologists, pathologists, and oncologists work in tandem to interpret findings that do not fit the “classic” presentation.

Key takeaways for the future of clinical practice include:
- Increased Vigilance: Atypical muscular lesions in patients with known or suspected malignancy should always prompt investigation for metastatic disease.
- Histological Priority: Imaging alone is often insufficient. Biopsy remains the gold standard for defining the treatment path.
- Personalized Staging: Recognizing rare metastatic patterns early allows for more accurate staging and prevents unnecessary, invasive procedures when systemic therapy is the more appropriate course of action.