Hypertension-induced heart damage often begins long before a patient shows symptoms or meets clinical diagnostic thresholds. According to the World Health Organization, 1.4 billion adults live with hypertension, yet current screening tools like standard echocardiography often fail to detect early myocardial remodeling. Emerging technologies, including speckle-tracking echocardiography and cardiac magnetic resonance (CMR) mapping, now allow clinicians to identify subclinical fibrosis and systolic dysfunction, potentially opening a window for reversible treatment before structural heart disease becomes permanent.
The Hidden Progression of Hypertensive Heart Disease
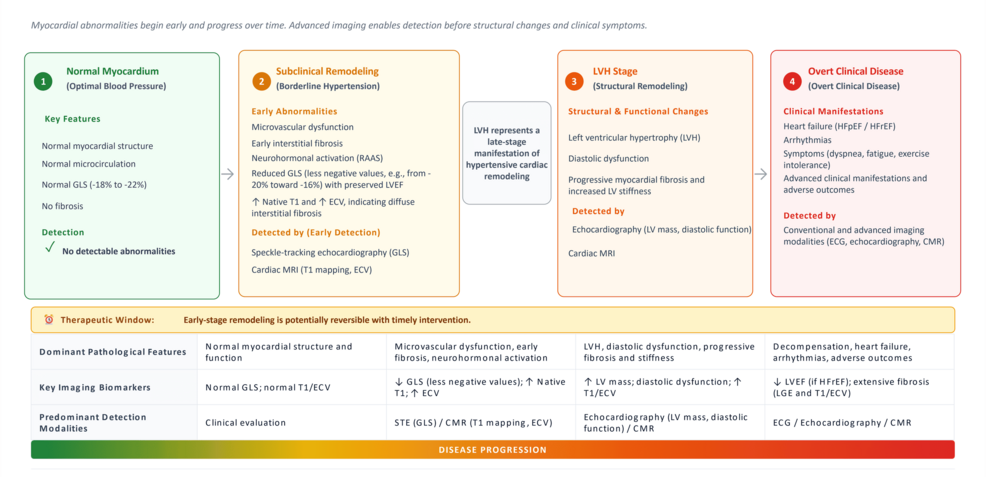
Hypertensive heart disease (HHD) is traditionally viewed as a structural transition from pressure overload to left ventricular hypertrophy (LVH). However, research indicates that myocardial damage occurs well in advance of detectable wall thickening. According to studies published in the field, processes such as interstitial fibrosis, microvascular ischemia, and neurohormonal activation begin while blood pressure is still in the “borderline” or “high-normal” range—defined by the 2024 European Society of Cardiology guidelines as 120-139/70-89 mmHg.
At this stage, the heart undergoes “subclinical remodeling.” The renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system trigger fibroblast activation, leading to collagen deposition in the interstitial space. Unlike later-stage scarring, this early-stage reactive fibrosis is partially reversible with targeted antihypertensive therapy, provided it is detected early enough to intervene.
Pro Tip: Don’t rely solely on standard blood pressure readings. If you are in the “borderline” hypertension category, ask your cardiologist about your global longitudinal strain (GLS) scores, which can reveal heart muscle weakness that isn’t visible on a standard ultrasound.
Why Conventional Imaging Often Misses the Mark
Standard tools like the electrocardiogram (ECG) and two-dimensional echocardiography have significant limitations in early detection.
While two-dimensional echocardiography remains the clinical workhorse, it relies on geometric assumptions that can lead to diagnostic errors. Because conventional metrics like ejection fraction (LVEF) remain normal until the heart is significantly damaged, they are poor indicators of the subtle, subendocardial dysfunction that defines the early phases of HHD.
Advanced Diagnostics: Speckle-Tracking and CMR
To overcome these gaps, medical centers are increasingly turning to advanced imaging techniques that look beyond basic structure.
- Speckle-Tracking Echocardiography (STE): This method tracks the movement of myocardial “speckles” to measure Global Longitudinal Strain (GLS).
- Cardiac Magnetic Resonance (CMR) T1 Mapping: This is currently the gold standard for detecting diffuse interstitial fibrosis. By measuring T1 relaxation times, clinicians can quantify collagen deposition in the heart muscle before it forms into a permanent scar (LGE), offering a quantitative look at the heart’s health that echocardiography cannot match.
Did you know? Artificial intelligence is being integrated into ECG analysis to predict subclinical LV dysfunction.
The Future of Integrated Screening
The next frontier in cardiology involves integrating these imaging markers with circulating biomarkers like NT-proBNP and high-sensitivity cardiac troponin. By combining anatomical data from CMR with biochemical indicators of myocardial stress, doctors can build a more precise risk profile for patients.
For low- and middle-income regions, where high-cost CMR is often unavailable, the strategy is shifting toward a tiered approach. Portable STE and AI-assisted ECGs serve as primary screening tools, reserving expensive CMR imaging for cases where definitive phenotyping is required. This precision-based approach aims to shift the focus from treating end-stage heart failure to preventing the initial structural changes that lead to it.
Frequently Asked Questions
Can hypertensive heart disease be reversed?
Evidence suggests that early-stage remodeling, characterized by reactive fibrosis and subclinical strain abnormalities, is partially reversible. Aggressive control of blood pressure using ACE inhibitors or ARBs has been shown to improve GLS values and reduce myocardial stress.
What is the difference between reactive and replacement fibrosis?
Reactive fibrosis is an early, diffuse expansion of the interstitial space that is potentially reversible. Replacement fibrosis is the result of cell death and forms permanent, focal scarring that cannot be reversed.
Is CMR always necessary for hypertension screening?
No. CMR is considered the gold standard for research and complex cases, but it is costly and time-intensive. Most clinicians utilize echocardiography and ECG for initial screening, reserving CMR for patients with unclear findings or when a more detailed tissue characterization is required.
Are you concerned about your cardiovascular health? Understanding the markers of early heart disease is the first step toward long-term protection. Schedule a consultation with a heart specialist today to discuss whether advanced imaging is right for your risk profile, or subscribe to our newsletter for the latest updates on cardiovascular screening and prevention.
Keep reading