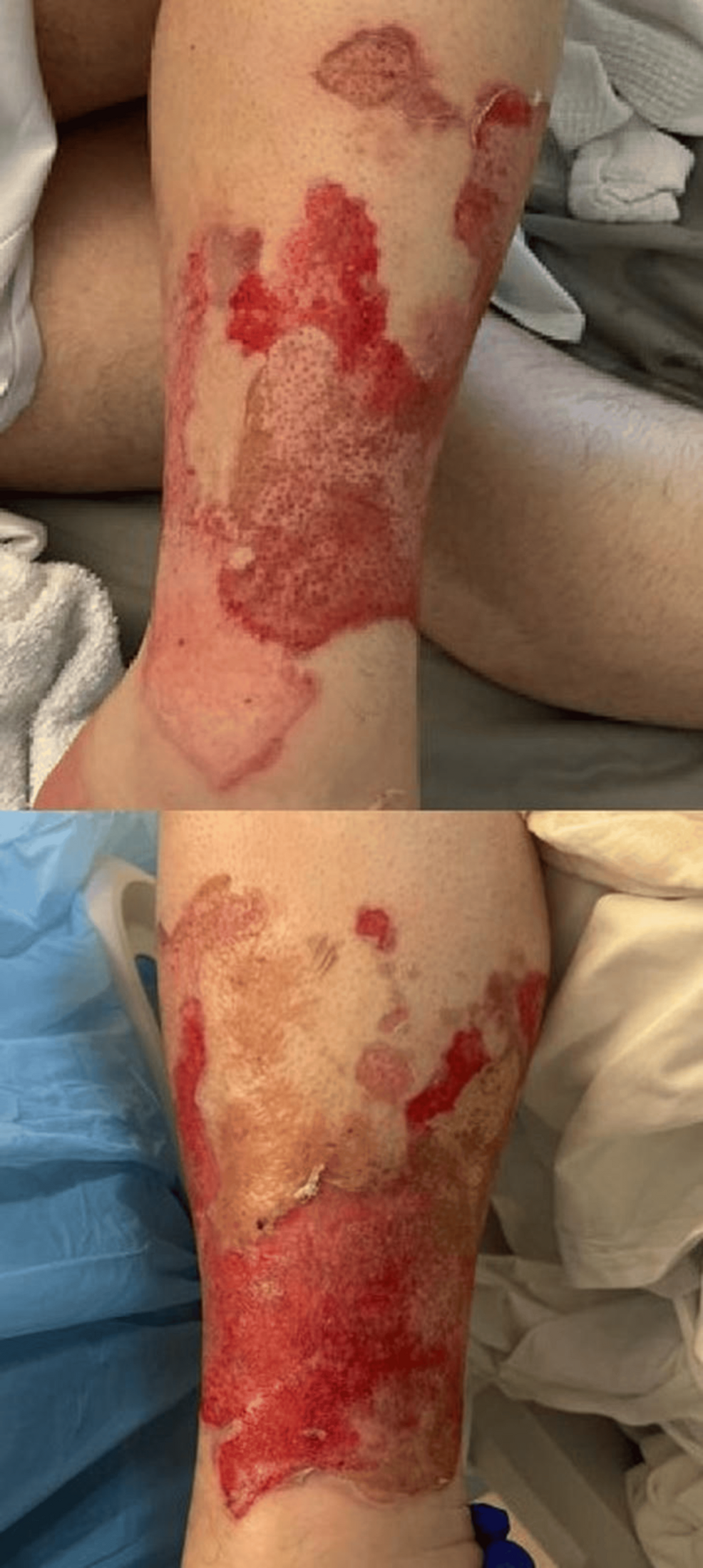
Non-suicidal self-injury (NSSI) during acute stimulant intoxication is increasingly recognized as a clinical phenomenon driven by the intersection of chronic somatic pain, trauma, and substance use. A recent case study describes a patient who ignited psoriatic plaques on his legs while intoxicated with cocaine, amphetamines, and other substances, citing a desperate need to relieve intractable pruritus and pain rather than suicidal intent.
The Intersection of Psoriasis and Addiction
Psoriasis, an immune-mediated inflammatory skin disease, affects roughly 2–3% of the global population, according to data cited by the authors of the Loyola University Medical Center case report. Beyond the physical lesions, the condition is linked to a 15% higher risk of self-harm compared to the general population. Research indicates a bidirectional relationship between the skin condition and substance use disorders; a Swedish study found that patients with psoriasis face a 4.3-fold increase in the risk of developing a new substance use disorder after their diagnosis, suggesting that some may turn to substances to cope with the chronic, burning pain of the disease.
Mechanisms of Pain-Relief-Motivated Self-Injury
The patient, a 34-year-old male, experienced severe pruritus and pain that became intolerable while under the influence of cocaine, amphetamines, cannabis, benzodiazepines, and alcohol. Psychiatrists who evaluated the patient determined the act was an impulsive, intoxication-driven attempt to stop the pain, rather than a suicide attempt. The medical team noted that the patient’s history of post-traumatic stress disorder (PTSD)—stemming from two significant motor vehicle accidents and childhood adversity—likely contributed to his emotional dysregulation and reduced distress tolerance.
The case highlights the “endogenous opioid model” of NSSI, where self-inflicted pain may transiently trigger the body’s opioid signaling, providing a temporary, albeit dangerous, sense of relief. In this instance, the patient’s use of stimulants likely exacerbated his hyper-awareness of somatic pain, creating a “feed-forward loop” of distress.
Integrated Care Strategies for Complex Patients
Treating patients with co-occurring inflammatory disease, trauma, and addiction requires moving beyond standard screening protocols. The clinical team at Loyola University Medical Center suggests that addiction treatment models must begin to incorporate:
- Dermatologic Assessment: Addressing the physical pain burden of skin conditions to prevent them from becoming triggers for self-injury.
- Trauma-Informed Care: Screening for PTSD and adverse childhood experiences that may impair a patient’s ability to regulate distress during periods of intoxication.
- Coordinated Treatment: Bridging the gap between dermatology, psychiatry, and addiction-focused psychotherapy to address the patient’s holistic needs.
Have you or a loved one struggled with the intersection of chronic pain and mental health? Share your thoughts or questions in the comments below, or subscribe to our newsletter for the latest updates on integrated health research.