The Complex Reality of Vitiligo-Like Depigmentation in Melanoma Treatment
Immunotherapy has revolutionized the management of advanced melanoma, providing new hope for patients with metastatic disease. Among the various responses observed during treatment with PD-1 inhibitors like nivolumab, vitiligo-like depigmentation (VLD) has emerged as a significant clinical phenomenon. While often viewed as a sign of a robust immune response, recent clinical evidence suggests the relationship between skin changes and long-term survival is far more nuanced than previously understood.
Understanding VLD and Immunotherapy
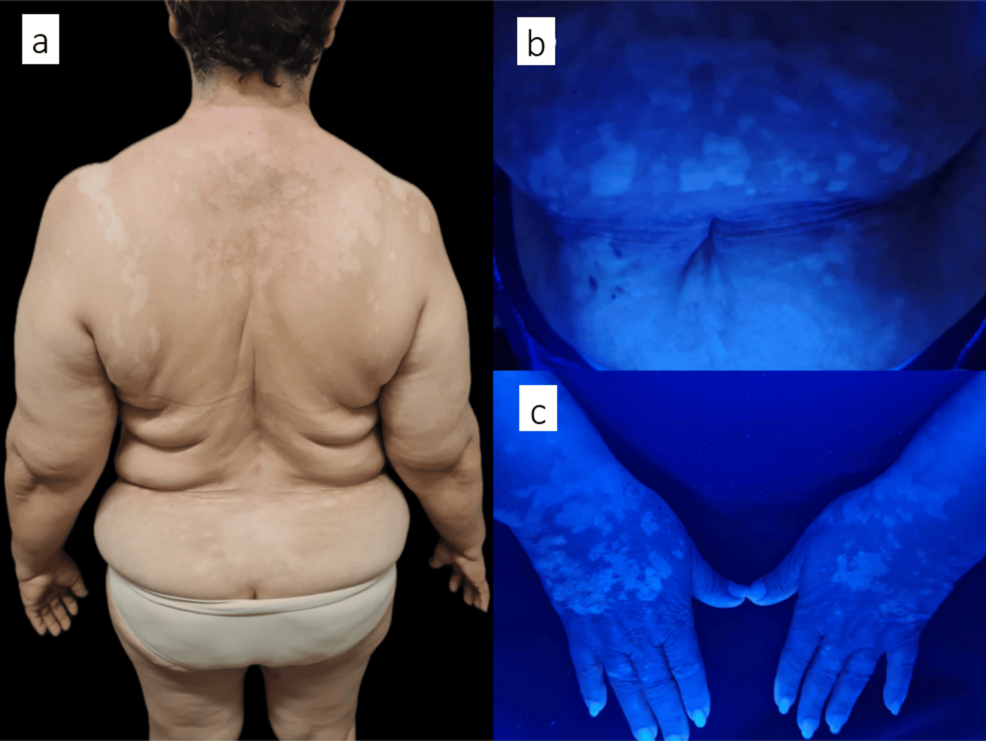
Vitiligo-like depigmentation is a cutaneous adverse event characterized by the loss of pigment in patches of skin. It occurs in an estimated 7.5% of melanoma patients undergoing nivolumab therapy. The condition typically manifests months after the initiation of treatment, appearing as confluent hypochromic macules on the face, trunk, and extremities.
VLD is thought to occur because the immune system, once activated by PD-1 inhibitors, may cross-react with antigens shared by both melanoma cells and normal melanocytes, leading to the destruction of pigment-producing cells.
When Skin Markers Don’t Predict Survival
Historically, medical literature has frequently associated VLD with favorable therapeutic outcomes. Some meta-analyses have even suggested a correlation between these depigmented patches and improved progression-free or overall survival. However, clinical experience shows that Here’s not a universal rule.
A notable case study involving a 72-year-old patient highlights this discrepancy. Despite achieving a complete radiologic response and developing extensive VLD after 11 cycles of nivolumab, the patient eventually experienced disease progression. Metastases were later documented in the liver, lungs, and central nervous system, proving that the development of VLD does not consistently predict sustained clinical benefit.
Clinical Implications for Future Treatment
The heterogeneity of patient responses to immunotherapy poses a challenge for clinicians. While VLD may serve as an immunologic marker of antitumor activation, it should not be considered an absolute guarantee of long-term success. The dynamic relationship between immune activity and tumor burden means that even patients who show classic signs of treatment response require vigilant, long-term monitoring.
Patients undergoing immunotherapy who develop new skin lesions should consult their oncology team immediately. While VLD is a known side effect, every change in skin appearance should be evaluated within the context of the patient’s broader clinical and radiologic status.
Frequently Asked Questions (FAQ)
- Is VLD a sign that my melanoma treatment is working?
While VLD has been linked to antitumor immune responses in many studies, it is not a foolproof predictor of success. As seen in recent clinical cases, disease progression can occur even after the development of VLD. - When does VLD typically appear?
VLD often develops months after treatment begins. Research indicates an average onset of approximately 6.9 months following the initiation of immunotherapy. - Should I stop treatment if I develop vitiligo-like patches?
No. VLD is a recognized adverse event, but it is often managed with photoprotection and skin care while continuing the primary cancer therapy. Always follow the guidance of your oncology team.
Are you or a loved one navigating a melanoma diagnosis? Subscribe to our newsletter for the latest updates on oncology research and patient care strategies, or explore our resource library for more in-depth articles on immunotherapy.
Worth a look