Navigating the “Stroke Mimic” Dilemma: Clinical Decisions Under Uncertainty
In the high-pressure environment of emergency neurology, the clock is the ultimate adversary. When a patient presents with a sudden, disabling neurological deficit, clinicians must act within a narrow therapeutic window. However, a recurring challenge remains: distinguishing an acute ischemic stroke from “stroke mimics”—conditions that present with similar symptoms but different underlying causes.
Recent clinical experiences highlight the complexity of this diagnostic tightrope. In cases of severe acute aphasia, the absence of clear neuroimaging—often due to patient agitation or technical limitations—forces a decision based on risk-benefit analysis rather than absolute diagnostic certainty.
The Role of Tenecteplase in Hyperacute Care
The use of thrombolytics like tenecteplase has become a cornerstone of stroke intervention. Evidence suggests that even when a patient is later determined to have had a stroke mimic, the rate of symptomatic intracranial hemorrhage following thrombolysis remains low. This clinical reality provides a defensible pathway for physicians to treat potentially disabling events when the alternative—withholding treatment—could lead to permanent disability if the stroke were real.

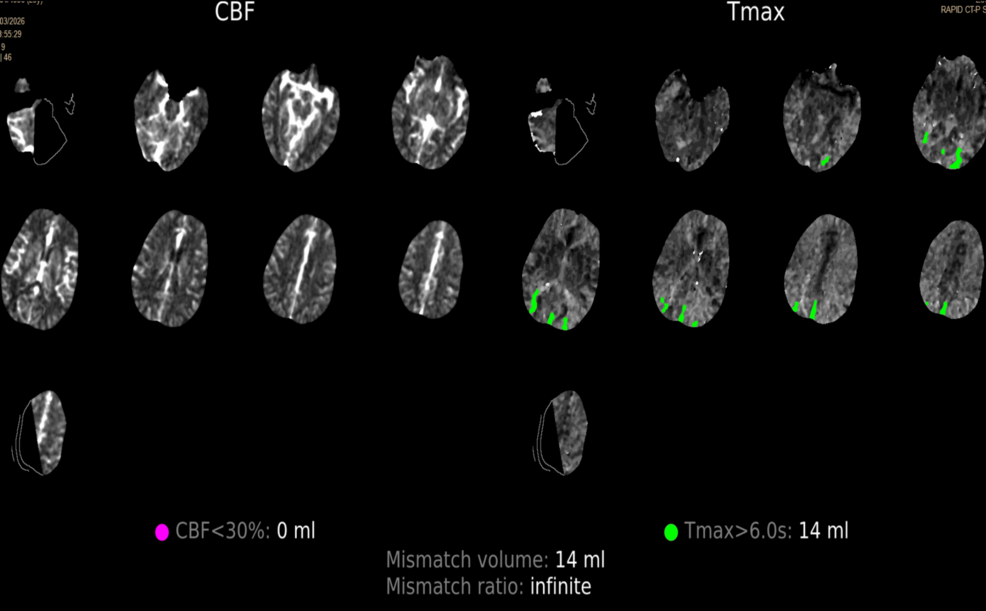
A recent case study involving a 29-year-old patient underscores this necessity. The patient presented with profound aphasia and sensory deficits. Despite inconclusive perfusion maps and motion artifacts in the CT suite, the clinical severity (NIHSS score of 5) and the therapeutic window justified the administration of 17.5 mg of IV tenecteplase. The patient made a complete recovery and subsequent follow-up suggested a diagnosis of migraine with aphasic aura rather than a stroke.
Post-Acute Diagnostic Reorientation
The journey does not end at the emergency department door. Cautious diagnostic reorientation is essential. In many cases, initial suspicions of stroke are refined through:
- Delayed Imaging: MRI sequences that show no diffusion restriction help rule out established infarction.
- Outpatient Monitoring: Tracking recurrent episodes can reveal patterns—such as responsiveness to naproxen—that point toward migraine-related phenomena.
- Differential Consideration: Conditions like HaNDL syndrome (Headache and Neurological Deficits with cerebrospinal fluid Lymphocytosis) or postictal aphasia must be considered, even if they remain unconfirmed due to patient preference or limited diagnostic data.
Future Trends in Emergency Neurology
As diagnostic technology evolves, the goal is to bridge the gap between “probabilistic” and “definitive” diagnosis. The future of stroke care likely involves:
- Enhanced Imaging Protocols: Reducing the time required for high-quality neuroimaging even in agitated patients.
- Biomarker Integration: Developing rapid blood-based tests that could potentially help distinguish ischemic events from mimics in the field.
- Structured Follow-up: Emphasizing the role of primary care and neurology clinics in refining diagnoses after the acute phase, ensuring that the “stroke mimic” label is supported by objective clinical evidence.
Frequently Asked Questions (FAQ)
What is a stroke mimic?
A stroke mimic is a medical condition that presents with symptoms similar to a stroke—such as speech loss or weakness—but is caused by something else, such as a migraine, seizure, or metabolic imbalance.
Why is thrombolysis given if it might be a mimic?
Because the risk of missing an actual stroke is high and can lead to permanent brain injury, clinicians often prioritize immediate treatment when the patient is within the therapeutic window and hemorrhage has been excluded via CT.
How do doctors confirm it was a mimic?
Confirmation usually happens post-acutely through normal MRI findings, lack of evidence of brain injury, and clinical follow-up that identifies recurrent, non-stroke patterns.
Are you a healthcare professional or a patient interested in the latest advancements in stroke care? Subscribe to our newsletter for the latest updates on neurology and emergency medicine, or explore our archives for more deep dives into complex clinical case studies.