The Bundibugyo virus disease (BVD) outbreak in the Democratic Republic of the Congo and Uganda has escalated significantly, with 534 confirmed cases and 93 deaths reported as of June 6, 2026. The World Health Organization (WHO) has declared a Public Health Emergency of International Concern (PHEIC) to address the rapid cross-border transmission and rising case numbers.
Will the outbreak continue to spread across borders?
Current epidemiological data suggests a high potential for regional spread. While the outbreak is currently concentrated in the Democratic Republic of the Congo (DRC) and Uganda, the WHO has assessed the risk for countries sharing land borders with these nations as high. This assessment is driven by sustained population mobility, particularly through cross-border trade and mining activities.
In Uganda, the situation is already showing signs of cross-border impact. As of June 6, 2026, Uganda has reported 19 confirmed cases, including two deaths in imported cases and one probable death. All cases in Uganda have been linked to travelers from the DRC or secondary infections. The WHO notes that the risk in Uganda remains high due to these ongoing epidemiological links along the eastern DRC–western Uganda corridor.
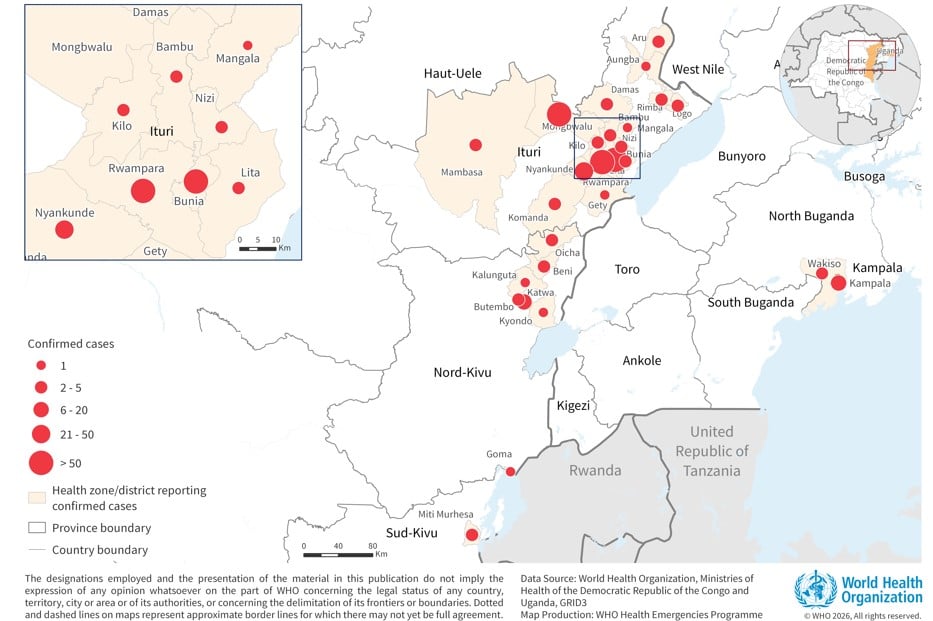
The scale of the outbreak in the DRC is substantial. The virus has been detected in 25 health zones across Ituri, North Kivu, and South Kivu provinces. Ituri Province remains the epicenter, accounting for 94% (487) of the confirmed cases in the DRC.
The Bundibugyo virus is a zoonotic disease. While it spreads person-to-person, fruit bats are suspected to be the natural reservoir in the wild.
How will funding gaps impact future containment?
The ability to suppress future transmission depends heavily on the mobilization of international resources. On June 5, 2026, the Africa Centres for Disease Control and Prevention (Africa CDC) and the WHO launched a joint continental preparedness and response plan. This plan includes a request for US$ 518 million to support African countries in detecting and responding to the outbreak.
Without this funding, several critical response activities could falter:
- Surveillance and Laboratory Capacity: Strengthening the ability to detect cases early.
- Infection Prevention and Control (IPC): Essential for protecting healthcare workers.
- Safe Treatment Centers: Setting up optimized environments for patient care.
- Community Engagement: Building trust to ensure safe burial practices and contact tracing.
Security-related incidents in the affected provinces are already creating operational hurdles. According to the WHO, these incidents constrain access for response teams, disrupt surveillance, and increase the risk of undetected transmission. If funding and security do not improve, the window for containing the virus may narrow.
What role will medical research play in stopping BVD?
A major challenge in managing this outbreak is the current lack of medical countermeasures. As of the latest reports, there are no approved vaccines or specific treatments available for Bundibugyo virus disease.
To address this, the WHO has convened technical advisory groups, including the Strategic Advisory Group of Experts (SAGE), to evaluate candidate vaccines and therapeutics. Future trends in the outbreak’s management will likely be dictated by how quickly these research efforts can translate into usable medical tools.
Clinical diagnosis also remains a hurdle. Because early symptoms like fever, fatigue, and muscle pain are non-specific, BVD can easily be mistaken for other endemic illnesses like malaria. This diagnostic delay can lead to increased transmission in healthcare settings if proper precautions aren’t taken immediately.
Because BVD symptoms mimic malaria, rapid laboratory confirmation using PCR or antigen/antibody-based assays is critical to prevent accidental exposure in clinical settings.
Comparing the Impact: Regional Disparities
The severity of the outbreak varies significantly by location, which may influence where future resources are concentrated. A look at the Case Fatality Rate (CFR) reveals a stark contrast:
| Region (DRC) | Case Fatality Rate (CFR) |
|---|---|
| Ituri Province | 15% |
| North Kivu Province | 64% |
| DRC Overall | 17.7% |
The significantly higher CFR in North Kivu compared to Ituri suggests that the virus may be behaving differently or that healthcare access varies between these provinces. This data will be vital for health authorities as they prioritize intervention strategies.
Frequently Asked Questions
What are the primary symptoms of Bundibugyo virus disease?
Early symptoms include fever, fatigue, muscle pain, headache, and sore throat. These can progress to gastrointestinal issues, organ dysfunction, and sometimes haemorrhagic manifestations.

Is there a travel restriction for the DRC or Uganda?
No. The WHO currently advises against any restrictions on travel to or trade with the Democratic Republic of the Congo or Uganda based on available information.
How is the virus spread between humans?
Transmission occurs through direct contact with the blood, secretions, organs, or other bodily fluids of infected individuals, or through contact with contaminated surfaces and items.
Stay Informed: The situation regarding the Bundibugyo virus is evolving daily. To receive the latest updates on global health emergencies and outbreak responses, subscribe to our newsletter or share this article with your network to spread awareness.
Related reading