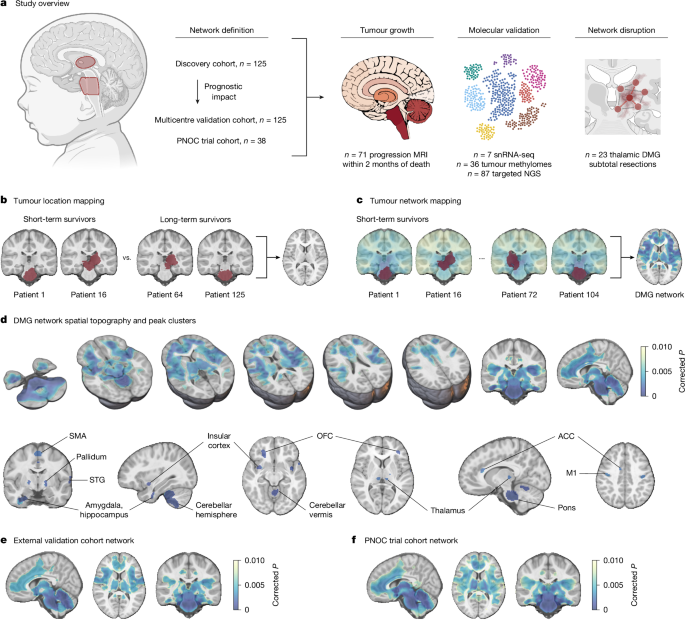
Researchers have identified a specific “DMG network” of brain connectivity that predicts survival outcomes for children with diffuse midline gliomas (DMG), including diffuse intrinsic pontine glioma (DIPG). According to a multi-institutional study led by Great Ormond Street Hospital (GOSH), mapping how these aggressive tumors integrate into the brain’s functional network allows clinicians to estimate patient prognosis with greater accuracy than tumor location alone. This discovery provides a new framework for understanding why some patients survive longer than others, potentially guiding future surgical and therapeutic interventions.
How does the DMG network predict patient survival?
The DMG network functions as a prognostic map, revealing that the impact of a tumor on overall survival depends on its specific functional connections to the rest of the brain. According to the study published by researchers at GOSH, the Children’s Hospital Colorado, and other international partners, patients whose tumors are more highly connected to this specific network face a higher risk of shorter survival. By calculating a “tumour network map score,” clinicians can stratify patients into risk groups, independent of standard clinical factors like age or sex. This method utilizes resting-state functional MRI (fMRI) and diffusion MRI (dMRI) data, treating the tumor not as an isolated mass, but as a node integrated into the brain’s complex wiring.

Researchers used data from 1,000 healthy children in the Adolescent Brain Cognitive Development (ABCD) study to create a “normative connectome,” which served as the baseline for mapping how these tumors hijack normal brain networks.
Why does tumor connectivity matter for surgical outcomes?
Understanding the “connectome”—the map of neural connections—allows surgeons to think about “connectomic resection.” According to the data, surgical procedures that prioritize the disconnection of infiltrated tumor networks may lead to better outcomes than simple volume reduction. By analyzing postoperative imaging, researchers found that the ratio of resected versus non-resected network connectivity serves as a potential biomarker for surgical success. This shifts the focus from how much of the physical mass is removed to how effectively the surgeon can isolate the tumor from the brain’s critical functional pathways.
What are the implications for future clinical trials?
The ability to predict survival based on network connectivity could refine how clinical trials are designed for DMG and DIPG. Currently, identifying long-term survivors is difficult, but the DMG network provides a quantitative tool to control for baseline risk in these trials. According to the study, this network remains robust even when accounting for different molecular subtypes and co-mutations, such as those in TP53 or BRAF. As researchers move toward personalized medicine, this connectivity-based approach offers a way to stratify patients more precisely, ensuring that experimental therapies are tested against a clearer understanding of the disease’s natural history.
When reviewing clinical trial data for pediatric neuro-oncology, look for mentions of “network mapping.” It is becoming a standard for assessing how tumors interact with the brain’s functional hierarchy beyond simple tumor size.
Frequently Asked Questions
What is a diffuse midline glioma (DMG)?
A DMG is an aggressive, infiltrative tumor that arises in the midline structures of the brain, such as the pons or thalamus. According to the 2021 World Health Organization criteria, these tumors are often H3K27-altered, a genetic marker associated with their rapid growth.

Can this connectivity mapping be used for adult brain tumors?
The researchers tested the specificity of the DMG network against two cohorts of adults with glioblastoma (GBM). They found that the prognostic impact of the DMG network was specific to the pediatric disease, suggesting that the way these tumors integrate into the brain is unique to the developing pediatric connectome.
How is the DMG network identified in individual patients?
Clinicians use high-resolution MRI data, including T1-weighted and T2-FLAIR sequences. These images are processed using software like ITK-SNAP to create a 3D mask of the tumor, which is then registered to a standard brain template (MNI space) to calculate its connectivity to the established DMG network nodes.
Are you interested in the latest advancements in pediatric neuro-oncology? Subscribe to our research newsletter for monthly updates on clinical trials and neuroimaging breakthroughs.
Keep reading