
The Rising Global Burden of Hypertension
Hypertension remains the leading “silent killer” worldwide, affecting more than 1.3 billion adults and accounting for roughly 10 million premature deaths each year [Murray et al., 2020]. The Global Report on Hypertension (WHO, 2023) highlights a growing prevalence in low‑ and middle‑income countries (LMICs), where health systems often lack the capacity to diagnose, treat, and monitor patients effectively.
Recent analyses of 87 risk factors across 204 countries show that uncontrolled blood pressure contributes to the largest share of disability‑adjusted life years (DALYs) among cardiovascular risk factors [Zhou et al., 2021]. This trend is especially stark in sub‑Saharan Africa, where hypertension awareness can be below 30 % and control rates under 10 % [Jobe et al., 2025].
Key Drivers
- Rapid urbanisation and dietary shifts toward processed foods.
- Limited access to affordable antihypertensive medication.
- Weak primary‑care infrastructure and fragmented care cascades.
Task‑Shifting: Community Health Workers (CHWs) on the Frontline
Task‑shifting—delegating specific clinical duties to CHWs—has emerged as a cost‑effective strategy to bridge workforce gaps. Systematic reviews confirm that CHW‑led hypertension care can improve detection by up to 30 % and modestly increase control rates [Lamloum et al., 2023].
Success Stories
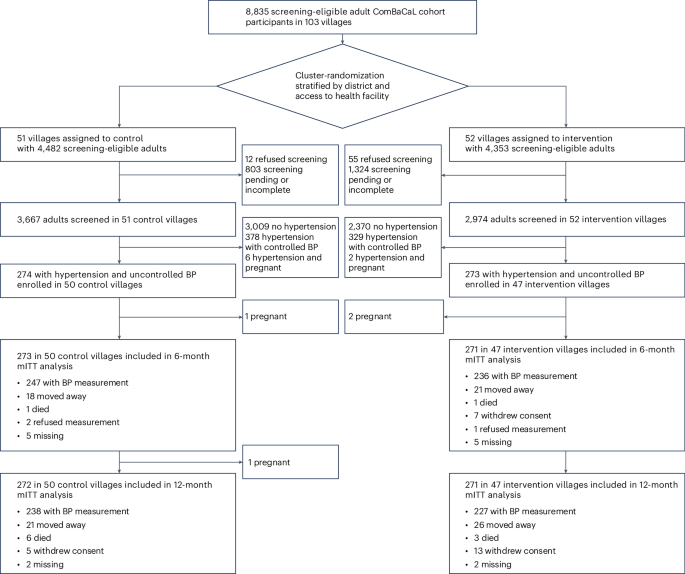
Lesotho’s ComBaCaL Cohort – Lay village health workers (VHWs) screened over 10 000 residents, identifying 2 800 modern hypertension cases and linking 70 % to care [Gerber et al., 2025].
India’s DISHA Study – Frontline workers delivered lifestyle‑modification counseling, achieving a mean systolic drop of 5 mm Hg across clusters [Kondal et al., 2022].
Digital Health: Mobile Decision Support & mHealth
Mobile health (mHealth) platforms are transforming how CHWs collect data, calculate cardiovascular risk, and deliver evidence‑based recommendations. The Community Health Toolkit (Medic Mobile, 2024) now offers offline risk‑chart calculators aligned with WHO’s 21‑region CVD risk models [WHO CVD Risk Charts, 2019].
Real‑World Impact
In a cluster‑randomised trial in rural China, a village‑doctor‑led mHealth intervention reduced uncontrolled hypertension from 45 % to 28 % within 12 months [Sun et al., 2022]. Similarly, a Kenyan home‑based CHW program leveraged SMS reminders to improve medication adherence, achieving a 12 % absolute increase in control rates [Mbuthia et al., 2024].
Innovative Care Models Shaping the Future
Beyond task‑shifting, hybrid models that combine community outreach, tele‑consultation, and pharmacy‑based distribution are gaining traction.
Examples
- Home‑Based ART for HIV – Lesotho’s VIBRA trial showed that CHW‑delivered ART refills maintained viral suppression comparable to clinic‑based care [Amstutz et al., 2021]. The same logistics can be repurposed for antihypertensive drug delivery.
- Cluster‑Randomised “HOPE 4” Adaptations – Integrated risk‑assessment, medication optimisation, and community education, cutting cardiovascular events by 20 % over five years [Hendriks et al., 2020].
Policy, Funding, and the Road Ahead
Global health agencies are prioritising hypertension within the Sustainable Development Goals. The WHO’s Global Strategy on Human Resources for Health: Workforce 2030 calls for scaling CHW programmes, while the Lesotho Community‑Based Health Policy 2024‑2029 earmarks $15 million for digital training tools.
Financing Trends
Public‑private partnerships are emerging as a catalyst. For example, the Global Burden of Disease consortium secured $120 million to fund data‑driven hypertension surveillance in 30 LMICs [Matsushita et al., 2025].
Frequently Asked Questions
- What is the most effective way to improve hypertension awareness in rural areas?
- Deploying CHWs equipped with mobile screening tools and community‑based education campaigns has consistently raised awareness by 20‑30 %.
- Can community health workers prescribe antihypertensive medication?
- In many LMICs, CHWs follow protocol‑driven algorithms that allow them to initiate first‑line therapy under physician supervision.
- How do digital tools help with medication adherence?
- SMS reminders, electronic pill‑boxes, and decision‑support apps provide prompts and track adherence, leading to 10‑15 % improvements in control rates.
- What are the cost implications of task‑shifting?
- Studies estimate a 30‑40 % reduction in per‑patient costs compared with physician‑only models, while maintaining comparable health outcomes.
Take Action Today
Whether you’re a public‑health manager, a clinician, or a policy‑maker, the evidence is clear: empowering community health workers with simple digital tools can dramatically shift the hypertension curve. Reach out to learn how your organisation can pilot a CHW‑led hypertension program, or subscribe for monthly insights on global NCD strategies.